What is Congenital Hyperinsulinism
What is Congenital Hyperinsulinism (CHI)?
Congenital Hyperinsulinism (CHI) is a rare but serious condition that affects how the body regulates blood sugar. It is the most common cause of persistent hypoglycaemia in infants and children. Understanding how CHI works, and why early diagnosis and treatment are so important, can help families, carers, and healthcare professionals support children living with this condition.
Hyperinsulinism is the inappropriate and unregulated insulin secretion in relation to the blood glucose concentration. It is the main cause of recurrent and persistent hypoglycaemia in infancy and childhood and is a major cause of hypoglycaemic brain injury.
Normally, blood glucose levels are regulated by insulin secretion, however, in Hyperinsulinism, the beta-cells of the pancreas release insulin inappropriately all the time causing low blood glucose levels (hypoglycaemia). The high levels of insulin prevent ketones being made and so the brain is not only starved of its vital fuel glucose, but also prevents ketone bodies being used as alternative fuels.
When the brain has no glucose or ketones to use as fuel then the child is at risk of seizures, loss of consciousness and even brain injury.
")
Alder Hey Hospital patient Guide to Hyperinsulinism:
What is Congenital Hyperinsulinism (CHI)?
CHI is the most frequent cause of severe and persistent hypoglycemia (low blood glucose) in newborn babies and children. It is characterized by inappropriate and unregulated insulin secretion from the pancreas. In CHI the beta-cells (cells in the pancreas) release insulin inappropriately all the time and insulin secretion is not guided by the blood glucose level (as occurs normally). The action of insulin leads to persistent and severe hypoglycaemia.
- Hyperinsulinism affects approx 1:28,389 babies in the UK and Ireland (2020 National Institute of Health).
- Although a rare condition Hyperinsulinism is the leading cause of persistent and severe hypoglycaemia in babies aged 0-3 months.
- It typically presents in the neonatal period, infancy and childhood.
- It can be transient *, persistent, mild or severe.
- So far, up to 26 genetic mutations have been identified along with links to other syndromes such as Beckwith Weidemann, Turner Syndrome and Kabuki Syndrome.
* Transient hyperinsulinaemic hypoglycaemia means that the increased insulin production is only present for a short duration and may be found in conditions such as:
- Intrauterine growth retardation
- Infants of diabetic mothers
- Infants with perinatal asphyxia
Transient hyperinsulinism can occur in infants with no predisposing factors such as those listed above. More research is needed to understand why transient hyperinsulinism occurs.
Some syndromes can also present in the newborn period with hyperinsulinaemic hypoglycaemia. In infants with Beckwith Weidemann syndrome, up to 50 per cent have been observed to develop hyperinsulinaemic hypoglycaemia. Other syndromes were CHI could be a feature include Turner Syndrome and Kabuki Syndrome.
Other causes of hypoglycaemia can include fasting, postprandial (after meals) including dumping syndrome and being protein sensitive, as well as being exercise induced.
Many children with Hyperinsulinism can suffer other issues in relation to the management of the condition such as fluid overload, cardiac/respiratory issues, infections, feeding issues (loss of orality), gastro-oesophageal reflux and feed associated problems such as intolerances and allergies.
For further information on Hyperinsulinism we recommend visiting the following websites:
Great Ormond Street Hospital
https://www.gosh.nhs.uk/conditions-and-treatments/conditions-we-treat/hyperinsulinism/
This Great Ormond Street Hospital video explains the mechanisms of Congenital Hyperinsulinism and how it affects blood glucose levels:
National Guidelines on Hyperinsulinism
For detailed information on the presentation, acute and immediate management of hypoglycaemia and how Hyperinsulinism is diagnosed we recommend reading the UK National Guidelines on Hyperinsulinism which can be found here:
https://www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2023.1231043/full
Focal vs Diffuse Hyperinsulinism
There are two forms of Hyperinsulinism:
Focal – where specific area/s of the pancreas are affected, these are known as small focal lesions. If these can be accurately identified and completely removed it may cure the condition.
Diffuse – affects the whole pancreas. Sadly if there is no response to medical management this will require the removal of almost the entire pancreas with a greater risk of longer term effects, such as diabetes or pancreatic insufficiency and hypoglycaemia can still remain.

For more information on the role of the pancreas see https://hyperinsulinism.co.uk/the-pancreas-insulin/
Neurodevelopmental Outcomes in CHI
The following information has been taken from the UK National Guidelines, please refer to them to see and click on the referenced research papers. https://www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2023.1231043/full
Abnormal neurodevelopmental outcomes are present in a significant number of children with both persistent and transient forms of CHI (96, 97) with frequency up to 48% in those with severe forms.
While it is important to prevent neuroglycopaenia, it is also important to assess developmental progress in follow up. A developmental follow up schedule alongside medical review will enable screening for early problems, thereby facilitating early referral to community services for rapid intervention.
Screening for neurodevelopmental outcomes could be undertaken from age one year (Appendix 6), although evolving abnormalities may present later and ongoing neurodevelopmental assessment should be considered, especially with parental concerns (98). In older children, and in those with screening deficits, standardised assessment of cognitive function may be required.
Brain imaging is not usually part of standard clinical review as anatomical abnormalities do not necessarily correlate with functional outcomes. However, in those with severe neuroglycopenia, visual cortical function loss or recurrent seizures, brain imaging may be helpful for review by paediatric neurologists.
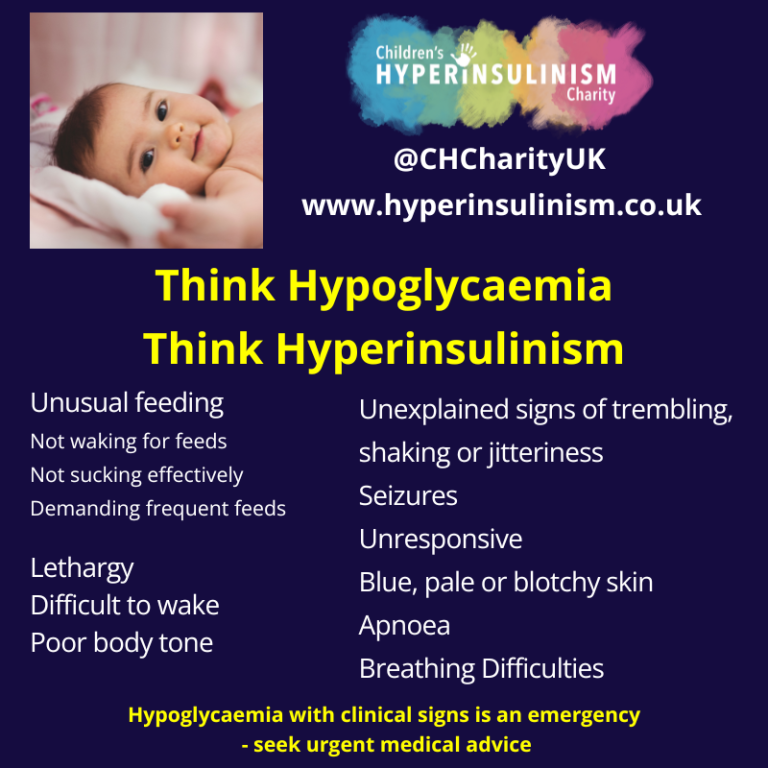
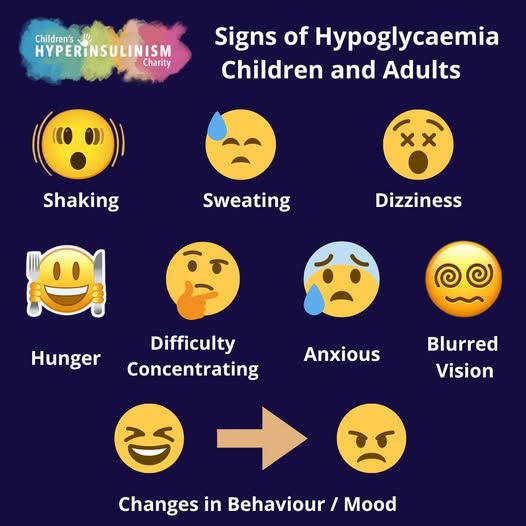
Recognising Hypoglycaemia in Babies and Children:
If you’re looking to understand more about how CHI develops and how it’s treated, we’ve created dedicated pages on :